
 In today’s parenting climate, having kids is not for the faint of heart. Parents, especially moms, are pelted with advice and recommendations: a “good” mom stimulates her children constantly, taking them to museums and signing them up for character-broadening extracurricular activities. She reads all the current literature on parenting. And she takes primary responsibility for the care and feeding of said children because, as psychology professor Holly Schiffrin notes, “we are the most qualified and you can’t trust anyone else, even husbands, because they won’t do it as well as we do.” It should go without saying that Schiffrin doesn’t necessarily believe that; she’s just summing up some women’s attitudes. But with the never-ending debate over how best to raise our children, it may be time to ask whether all this emphasis on “intense mothering” is making moms unhappy. That’s exactly what Schiffrin and colleagues at the University of Mary Washington, in Fredericksburg, Va., did, looking at whether women who endorse what they call “intensive parenting” beliefs — namely that women parent better than men and that children, viewed as sacred and fulfilling, should rightly be the center of a woman’s world — struggle more with mental health. Their conclusion? Women who insist “mother is best” are less satisfied with their lives. There’s even a term for when intensive parenting results in amped-up stress and guilt: the parenthood paradox. And, undoubtedly, you’ve seen the much-scrutinized piece in the Atlantic musing about women “having it all.” All of it “is saying the way we’re parenting today is taking a toll on women,” says Schiffrin, a study co-author. “We need to find that happy medium — all things in moderation. Yes, you need to be involved with your kids, but the standard we’re holding ourselves to is probably unachievable.” For their study, published recently in the Journal of Child and Family Studies, the researchers relied on a measure of intense mothering, which they developed. It included five categories: stimulation of the kids; the view that mother is best, which the researchers called “essentialism”; the belief that child-centered parenting is really different from two generations ago when children were to be seen and not heard; the idea that children are sacred and should bring joy and love to their parents; the premise that parenting is challenging and exhausting. The researchers looked at 181 moms of kids age 5 and under, and asked them to fill out an Internet questionnaire measuring their opinions about intensive mothering. Even after controlling for social support — help from Grandma, for example — researchers found that intensive mothers were not as happy. Moms who believe parenting is challenging and requires expert knowledge and skills were more stressed and more depressed than moms who didn’t think an arsenal of expertise was mandatory. Moms who think stimulation is necessary and that children are sacred did not show differences from other moms, which surprised Schiffrin. It could be because the “challenging” measure “tended to gobble up the other explanations,” she said. It’s important to note that intensive mothering is not necessarily the province of stay-at-home moms. Whereas the stay-at-home contingent buys into the belief that they have to be hands-on, working moms tend to think that stimulation is paramount. “It’s quantity vs. quality,” says Schiffrin. Truth be told, there’s likely some intensive mothering going on within all of us, at least to some degree. We talk about the importance of having downtime, yet we feel obliged to sign our kids up for a merry-go-round of basketball training–dance classes–piano lessons–chess club–sewing instruction because we’re convinced it’s good for them. And, quite possibly, because their friends are doing it and we don’t want our kids to miss out. Yet, as author Judith Warner observed on Healthland’s partner blog Ideas, this concept of parenting as a competitive sport doesn’t apply to all socioeconomic brackets: As Middlebury sociologist Margaret Nelson has written, parents of “lower educational and professional status” tend to have a very different style of interacting with their children — setting more “nonnegotiable limits” for example, investing a whole lot less in the cultivation of their children’s potentially limitless emotional and intellectual unfolding. This is not (just) because the lower-status women have different sorts of life demands pressing upon their time and other resources; it’s because they have a different idea of good motherhood, one that appears, perhaps, to offer some protection against the perfectionist misery of so many middle- or upper-middle-class moms. It’s also worth reiterating that women who subscribe to this exhausting parenting philosophy — and their numbers are not few — do so because they believe it benefits their children. Next year, Schiffrin hopes to look at whether intensive mothering actually conveys advantages to kids. “A lot of research says children of depressed mothers don’t fare as well,” she says. “If this ideology is making us depressed, it may not benefit kids in the long run.” After so much effort, wouldn’t that outcome be ironic? This article was written by Bonnie Rochman and appeared on Time.com: http://healthland.time.com/2012/08/07/mother-is-best-why-intensive-parenting-makes-moms-more-depressed/ photo by Jamie Grill / Iconica / Getty Images
0 Comments
 Tuesday, August 29th from 10am to 12pm, the Happy Camp Community Center, located at the 38 Park Way, will be distributing commodity boxes to income qualifying residents. Seniors 60+ who qualify will receive additional boxes and food supplies. Supplies are limited, first come first served.
 Posted Aug 25, 2017 on www.physiologytoday.com, article by Jean M Twenge Ph.D.
To read the entire article, "Why are so many teens depressed?", click here. For article highlights, read on… Around 2012 to 2013, there was sudden uptick in teens saying they were experiencing symptoms of depression—feeling hopeless, not enjoying life, believing they can’t do anything right. Depressive symptoms continued to increase over the next few years, making today's teens—whom I describe in my new book, iGen—significantly more depressed than teens just a few years before. As I found when I dug deeper, the increase in depressive symptoms was only part of the story. Happiness—which had been increasing among teens for 20 years—began to decline. Loneliness spiked sharply, and more entering college students (in the national American Freshman survey of 9 million students) said they felt depressed and overwhelmed. Even more concerning, 50% more teens in 2015 (vs. 2011) demonstrated clinically diagnosable depression in the NS-DUH national screening study. (It's important to note that all of these sources are surveys of unselected samples of teens, and notthose who seek treatment—thus they cannot be explained by greater treatment-seeking). The teen suicide rate tripled among girls ages 12 to 14 and increased by 50% among girls ages 15 to 19. The number of children and teens hospitalized for suicidal thoughts or self-harm doubled between 2008 and 2015. iGen'ers were experiencing a mental health crisis. As if that weren’t enough, no one seemed to know why. Economic causes seemed unlikely; the U.S. economy improved after 2011. It wasn’t academic pressure; in the MtF surveys, teens in the 2010s say they do fewer hours of homework than teens did in the 1990s, and the time college-bound high school students spend on extracurriculars--contrary to popular belief--is about the same in the American Freshman survey. There was no cataclysmic event or political shift during that time (these data predate Trump). Factors such as income inequality and shifting family structure, mentioned by some, had been building for decades, with no sudden shift in the 2010s. So what was it? Then it hit me. In another project, I’d found teens were spending less time with their friends in person and more time communicating electronically, with these trends accelerating after 2011. That, I realized, was around the time that smartphones became ubiquitous—when many teens (and adults) started spending nearly every waking moment looking at the phones in their hands. Sure enough, the Pew Center found that the percentage of Americans owning a smartphone crossed 50% in late 2012. That was also around the time social media became almost mandatory for teens. Smartphones and social media were also something that affected teens directly—a fundamental change in how they spent their time, not just an event in the news or a trend they heard about from their parents. So the time sequence fit—right when smartphones became common and teens started spending less time face-to-face, their psychological well-being plummeted. The next question was whether smartphones might be linked to lower well-being among individuals. In my analyses of MtF and the CDC's Youth Risk Surveillance System data for the book, I found they were—teens who spent more time on screens were less happy, more depressed, and had more risk factors for suicide. Those links remained when possible confounding factors such as gender, race, and socioeconomic status were taken into account. [A study] randomly assigned adults to give up Facebook for a week, or not. Those who gave up Facebook ended the week happier, less lonely, and less depressed. Not only that: No one disputes that in-person social interaction is linked to better mental health. So even if we dismiss the correlation between social media and depression—say, calling it neutral—the decline in in-person social interaction could certainly account for the increase in depression and unhappiness. And why has in-person social interaction declined? Probably because screen time increased. None of this means you should yank the smartphone out of your teens’ hands. As other studies have also documented, moderate use of smartphones (around an hour a day) is not harmful. In my analyses of data from the Youth Risk Surveillance System survey administered by the CDC, negative effects on mental health appeared only after two or more hours a day of use. Of course, most teens (and many adults) use their smartphones much more than two hours a day (the average is six to eight hours during leisure time), so it makes sense to consider setting limits. [It is not] OK that 50% more teens suffered from major depression in 2015 vs. just four years before. It is not OK that the suicide rate for teen girls is at its highest level since 1975. It is not OK that twice as many children and teens are now hospitalized for self-harm or suicidal thoughts. It is not OK that more teens say that they are lonely and feel hopeless. Given the undeniably negative trends in teens' mental health and the evidence suggesting smartphone use is at least partially behind them, it makes sense to limit kids' and teens' smartphone use. As with any intervention, the risks of doing something vs. doing nothing must be considered. There doesn't seem to be much risk involved in limiting smartphone use to 90 minutes a day or less. However, doing nothing and having teens continue to spend 6+ hours a day with new media risks having these negative mental health trends continue. For Help If you are struggling with depression, please visit the Happy Camp Community Center. We are open Tuesday through Thursday from 9am to 4pm; we can refer you to Siskiyou County’s Behavioral Health Services. Alternatively you can contact SAMHSA’s National Helpline at 1-800-662-HELP (4357).  The original article, by Sarah Stevenson, was posted on May 5, 2017, Senior Living Blog at aPlaceForMom.com. To read the entire article click here.
Feelings of loneliness and isolation can lead to serious consequences for senior health. Understanding the causes and risk factors for senior isolation can help us prevent it. Statistics on Senior Isolation According to the U.S. Census Bureau 11 million, or 28% of people aged 65 and older, lived alone at the time of the census. As people get older, their likelihood of living alone only increases. Additionally, more and more older adults do not have children, reports the AARP, and that means fewer family members to provide company and care as those adults become seniors. While living alone does not inevitably lead to social isolation, it is certainly a predisposing factor. Yet another important consideration is how often seniors engage in social activities. Statistics Canada reports that 80% of Canadian seniors participate in one or more social activities on a frequent basis (at least monthly) – but that leaves fully one-fifth of seniors not participating in weekly or even monthly activities. Social contacts tend to decrease as we age for a variety of reasons, including retirement, the death of friends and family, or lack of mobility. Regardless of the causes of senior isolation, the consequences can be alarming and even harmful. Even perceived social isolation – the feeling that you are lonely – is a struggle for many older people. Fortunately, the past couple of decades have seen increasing research into the risks, causes, and prevention of loneliness in seniors. Here are 20 facts about senior isolation to help you stay informed: 1. Senior isolation increases the risk of mortality. 2. Feelings of loneliness can negatively affect both physical and mental health. 3. Perceived loneliness contributes to cognitive decline and risk of dementia. 4. Social isolation makes seniors more vulnerable to elder abuse. 5. LGBT seniors are much more likely to be socially isolated. 6. Social isolation in seniors is linked to long-term illness. 7. Loneliness in seniors is a major risk factor for depression. 8. Loneliness causes high blood pressure. 9. Socially isolated seniors are more pessimistic about the future. 10. Physical and geographic isolation often leads to social isolation. 11. Isolated seniors are more likely to need long-term care. 12. Loss of a spouse is a major risk factor for loneliness and isolation. 13. Transportation challenges can lead to social isolation. 14. Caregivers of the elderly are also at risk for social isolation. 15. Loneliness can be contagious. 16. Lonely people are more likely to engage in unhealthy behavior. 17. Volunteering can reduce social isolation and loneliness in seniors. 18. Feeling isolated? Take a class. 19. Technology can help senior isolation – but not always. 20. Physical activity reduces senior isolation. Remember, understanding the causes and risk factors for senior isolation can help us prevent it. If you or someone you know are feeling depressed, please visit the Happy Camp Community Center. We contract with Siskiyou County Behavioral Health and can refer you to their services. We located at 38 Park Way in Happy Camp and are open Tuesday-Thursday, 9am to 4pm. 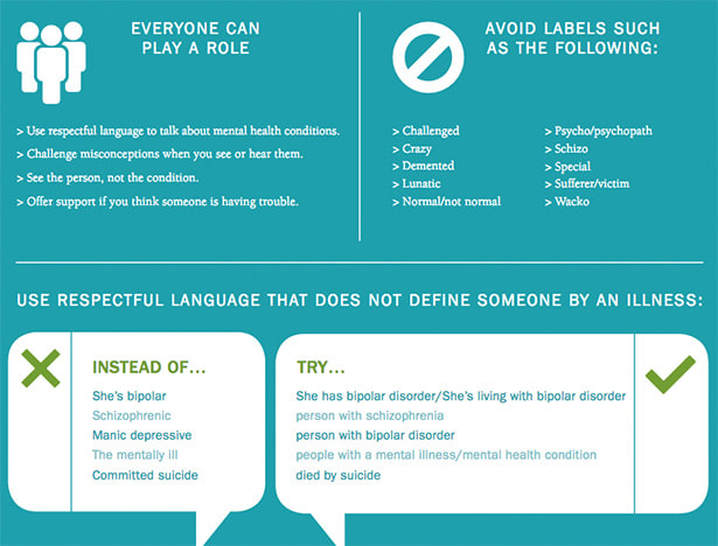 The need to eliminate stigma is nothing new. Fifteen years ago, a U.S. Surgeon General’s Report on Mental Health—the first and only one to date—identified stigma as a public health concern that leads peoples to “avoid living, socializing or working with, renting to, or employing" individuals with mental illness. Thanks to stigma, people living with mental health conditions are:
Many people living with mental health conditions don’t feel comfortable talking to their friends and family about what they’re dealing with. Those living with a mental health condition don’t want it any more than a person would want a broken leg. But focused thought and effort can’t make depression go away, just as focusing on healing won’t fix a shattered bone. Even worse, individuals living with mental illness often internalize the stigma that exists in our culture, damaging hopes for recovery. Some don’t seek treatment from a mental health professional. Their conditions worsen because they aren’t receiving the support and care they need to recover. And too often people take their own lives because they aren’t told by anyone that they’re not alone, they can recover and there is hope. To change this harmful status quo, NAMI (National Alliance on Mental Illness) is asking everyone to take our StigmaFree Pledge. Building a movement for change will require commitments from individuals, businesses, organizations, campuses and churches, as well as others. Once you’ve taken the pledge, consider all the ways you can live StigmaFree in your daily life. Maybe you can begin by being aware of the language you use or by choosing to be open or by deciding to learn more about mental illness. Every day brings new hope. Every day, we have an opportunity to help create broader understanding of mental health, overcome stereotypes and break down barriers. We can all do a little bit more each day to eliminate stigma and replace it with help and hope. So, help NAMI spread the word. Take the StigmaFree pledge and encourage your family and friends to do the same. This initiative, this movement is our attempt to reverse the harmful effects of stigma. So, when you hear someone using stigmatizing language, correct them. If you see someone using misleading stereotypes, educate them. And never forget to see people for who they are, not for how they act during their darkest days. Together, we will turn the tide on stigma by spreading awareness, support and understanding for every person who experiences mental illness. Together, we can make a difference for the better. |
AboutHappy Camp Community Action, Inc. is a Non-profit organization dedicated to economic development and youth programs in Happy Camp, California and surrounding communities. Archives
January 2020
Categories |
SERVICES |
Company |
Apart from the free survey software, we also have access to QuestionPro's free survey templates. We've
found many of them useful and powerful to collect insights from various stakeholders of our organization |
 RSS Feed
RSS Feed